Why Your VO2 Max Isn't Improving (The Oxygen Cascade Explained)
If your VO2 max has stalled, the reason is almost certainly that you are training the wrong step of the chain.
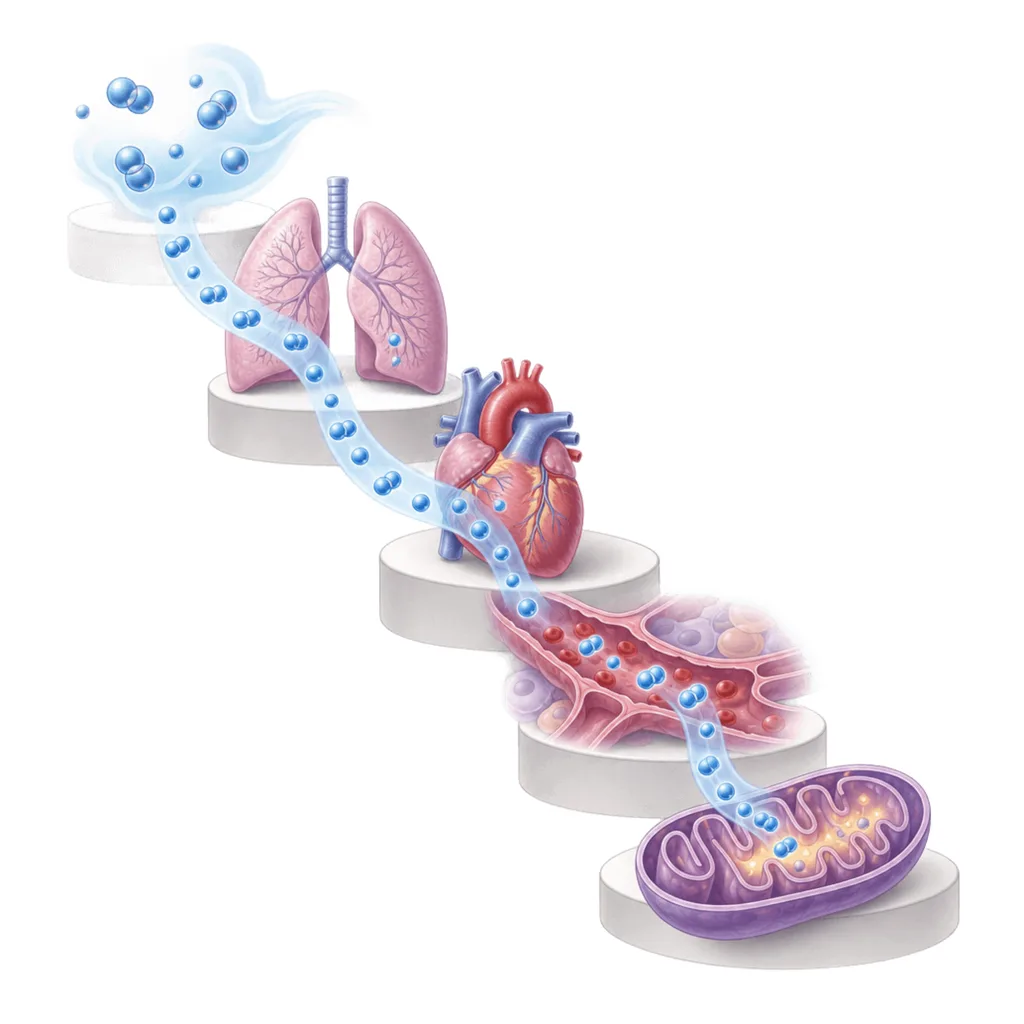
Oxygen takes five steps to get from the air to your muscles. Lungs, heart, blood, capillaries, mitochondria. Your VO2 max is set by whichever of those steps is narrowest and for almost every athlete it is the same one: how much oxygenated blood your heart can pump per minute. That is a delivery problem not a muscle problem. The training that best develops delivery is not the training most athletes think of for when they want a bigger VO2 max.
Here is the cascade, step by step with details about what each one actually responds to.
Your lungs are not the problem
Air comes in, oxygen crosses into the blood and blood leaves your lungs almost fully loaded. In a healthy athlete at sea level, arterial blood is around 97 to 98 percent saturated even at maximal effort.
There is almost no headroom there. You cannot train your lungs to load more oxygen into blood that is already nearly full. Lung capacity does not meaningfully expand with endurance training and it does not need to. Your lungs are overbuilt for the job.
Two exceptions worth knowing. At altitude, oxygen loading does become limiting. And some elite endurance athletes develop exercise induced arterial hypoxaemia, where cardiac output is so high that blood moves through the lungs too fast to fully saturate. If you are reading this at sea level and you are not a national level endurance athlete then your lungs are not what is holding you back.
Your heart is where VO2 max is won and lost
This is the step that matters. Cardiac output is how much blood your heart pumps per minute, and it is the product of two things: heart rate and stroke volume.
Maximum heart rate is essentially fixed. It does not rise with training, it drifts down slightly as you get fitter and it declines with age regardless of what you do.
Which leaves stroke volume, the amount of blood ejected with each beat. That is the single most trainable component of your VO2 max and it is where the differences between athletes live. When researchers compare people with different VO2 max values, the difference tracks maximal cardiac output. Since max heart rate is fixed, that means it tracks stroke volume.
Endurance training raises stroke volume three ways. The left ventricle becomes larger and more compliant, so it fills with more blood between beats. Blood and plasma volume expand, so there is more blood returning to fill it. And contractility improves, so more of what fills gets ejected.
That is the step to train.
Your blood decides how much oxygen each beat carries
Cardiac output moves the blood. Haemoglobin decides how much oxygen that blood is carrying.
Total haemoglobin mass tracks closely with VO2 max. It explains a large share of the difference between trained and untrained athletes and a meaningful part of the difference between men and women. Legitimately, endurance training expands plasma volume quickly, within days to weeks, and red cell mass more slowly over months. Altitude exposure works on this step too. It is trainable, takes time and responds to consistent aerobic volume rather than to any single session type.
Capillaries and mitochondria decide how much of your engine you can use
The last two steps are peripheral. Capillaries distribute blood to the muscle fibres and give red cells time to offload oxygen. Mitochondria consume it.
Here is the counterintuitive part. Your muscles' capacity to take up and use oxygen actually exceeds your heart's capacity to deliver it. When researchers isolate a small muscle group and remove the delivery constraint, that muscle can consume far more oxygen than the whole body VO2 max would predict. The mitochondria are not the main limiter of VO2 max. Delivery is.
But mitochondrial density and capillary network are what determine your lactate threshold, which is the fraction of your VO2 max you can actually hold. That is a different question from how big your ceiling is, and for most race distances it matters more. We wrote about that distinction in what an elite Hyrox athlete's lactate profile actually looks like.
Both of these adapt strongly to aerobic volume. Both detrain fast. One bed rest study found 42 days of inactivity cut total capillary length by 22 percent.
Does HIIT actually improve your VO2 max?
Yes and if you are untrained it is the fastest and most time efficient way to do it. A meta-analysis of 53 randomised controlled trials found that even short, low volume HIIT produces clear VO2 max gains in the general population. This is real. It is why HIIT is popular and it is why it works.
But time efficient is not the same as maximal, and the same meta-analysis is specific about that. The largest effects came from longer intervals of two minutes or more, higher work volume of at least fifteen minutes, and longer training periods of four to twelve weeks and beyond. Even inside the HIIT literature, more aerobic work sustained for longer beats it.
The early gains come easily because an untrained heart has a lot of stroke volume to gain and gets it from almost any hard stimulus. Once that is banked, the next increment comes from the slow stuff: ventricular remodelling, plasma and red cell expansion, capillary growth. Those are volume adaptations. They accumulate over months and years of mostly easy aerobic training, which is exactly why elite endurance athletes spend around 80 percent of their training below threshold.
The type of intensity that helps also shifts as you train. In well trained athletes, longer aerobic intervals such as the Norwegian 4x4 outperform short sprint intervals for VO2 max. So intervals keep their place. They just become a smaller and more specific lever than their popularity suggests.
The mistake is assuming that because HIIT gave you fast early gains, more and harder HIIT is the path onward.
What we see in our own athletes
This is not just theory and it shows up in our testing data.
Tayla came back from injury with her anaerobic threshold dropped to 12.7 km/h. She trained it with one Norwegian 4x4 session per week, four intervals of four minutes hard with four minutes recovery. Sixteen minutes of hard work a week, on top of her normal easy aerobic running. Eight weeks later her anaerobic threshold was 14.3 km/h.
Now look at what her aerobic threshold did over the same eight weeks. It moved from 11.5 to 11.9 km/h. Four tenths of a kilometre per hour.
That is the whole argument in one athlete. The intervals sharpened the top end, and they sharpened it hard, 1.6 km/h in eight weeks. The base underneath barely shifted. Sixteen minutes of weekly intensity is a sharpening tool not a basebuilding tool.
Now the other end of the spectrum. When we tested an elite Hyrox athlete, the standout feature of his profile was an exceptionally high aerobic threshold. His blood lactate stayed low across an extremely wide range of speeds at paces that would have most athletes accumulating. That is not something eight weeks of intervals produces. That is years of consistent aerobic volume, accumulated long before he was racing at the front.
Which step is limiting you?
The awkward part is that the cascade has a different narrowest step in different people.
One athlete is delivery limited. Their ceiling is low and the work is to build the engine: volume, stroke volume, blood, capillaries. Another has a big ceiling but cannot use much of it. Their VO2 max is fine and their lactate threshold sits at a low fraction of it, which means the problem is utilisation, not delivery. Those two athletes need almost opposite training and they cannot tell which one they are by feel or from a watch estimate.
A lactate threshold test tells you what fraction of your engine you can hold and whether your base is actually developing. A VO2 max test tells you how big the ceiling is. Together they tell you which step of the cascade is your limiter, and therefore what to train.
We measure thresholds from blood lactate at Team Rees in Caerphilly, KORE in Newport, UFIT in Cardiff, with Kulture in Bristol coming soon. VO2 max testing by gas exchange is launching shortly, which will let us measure the ceiling directly alongside the fraction you can use.
Book a lactate threshold test at Team Rees, Caerphilly, or KORE, Newport.
For more on what your thresholds tell you, read Your Zone 2 Heart Rate Is Probably Wrong and How Quickly Can You Improve Your Lactate Threshold?.
Ready to find your lactate threshold?
Book a test at one of our partner gyms and get a personalised training zone report.
Book a Test